- Health in Perspective
- Posts
- The Economics of Illness
The Economics of Illness
Market Incentives and Pharmaceutical Drug Development
Vinay Sudarsanam
March 06, 2025

“How does the capitalist system in the U.S. affect healthcare access and outcomes?” As soon as this question was asked in a recent fishbowl discussion I participated in, my hand shot up, for I could list so many issues with the current U.S. healthcare system. My answer began with, “in the U.S, the delivery of quality and timely healthcare is determined by aligning incentives.”
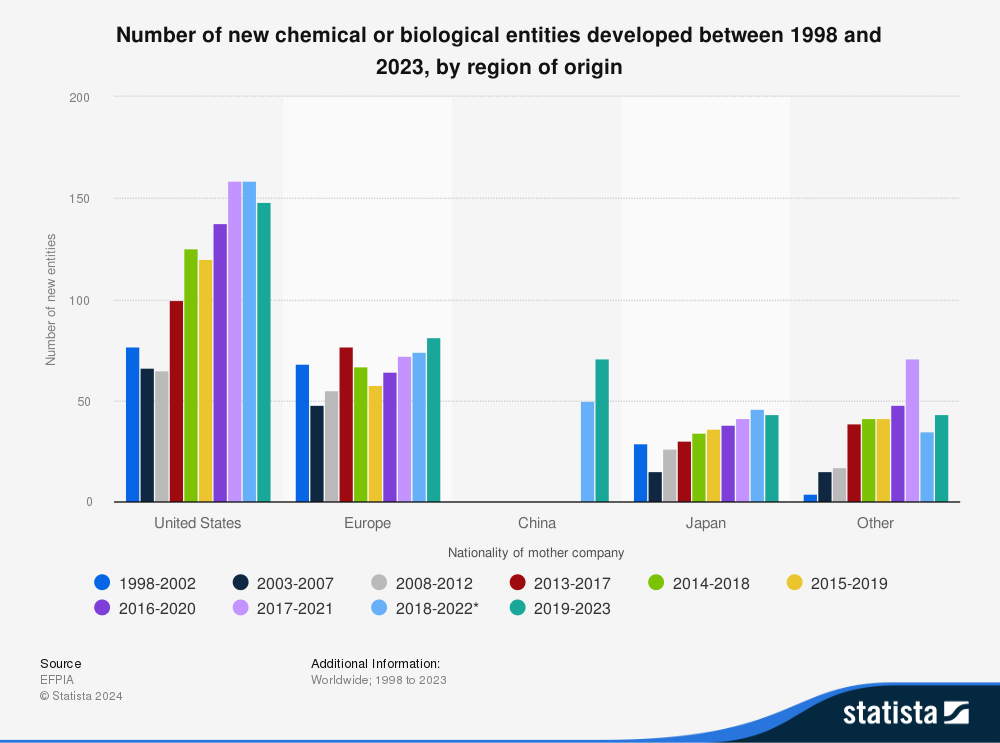
In a capitalist system, institutions are profit-oriented, willing to buy or sell in the market if the act results in a profit. While this profit-oriented system has resulted in significant innovation, specifically with pharmaceuticals (a large portion of new pharmaceuticals were developed in the U.S. and have been for the past 3 decades), it has also resulted in gaps in access to quality care when the interests of private industry did not align with those of patients. (1)
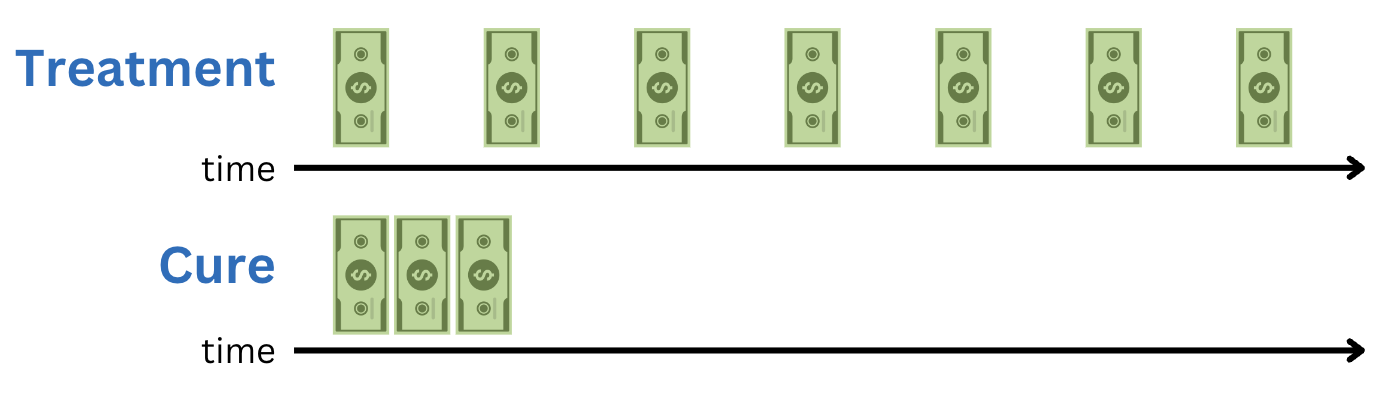
Over the past several years, new health economics research has focused on this new issue -- does the capitalist system in the U.S. hinder development of disease cures? (2) Producing therapies which patients must consume week after week, month after month, provides the producing firm with a steady revenue stream whereas a cure, by definition, requires consumption for a limited time, perhaps resulting in limited profits.
Let’s start with the patient perspective. If we think about some of the most expensive-to-treat uncured diseases, from Alzheimer’s to cardiovascular disease to cancer, of course, from a critical lens we begin thinking about the root causes of disease and the social determinants from access to healthy food, access to exercise opportunities, and access to quality low-cost healthcare, that play a role in disease prevalence and longer-term outcomes. However, in our modern medicalized society, we, and other healthcare stakeholders, often see the solutions to disease as pharmaceuticals or medical/surgical interventions. As patients, we want to see diseases cured such that in the event that we or someone we know develops that disease, we can be certain that a positive health outcome will be obtained.
However, the producer perspective does not necessarily reflect these same values. Pharmaceutical firms strive for continuing profitability for investors and to protect their bottom line. (2) Furthermore, with an average cost of pushing a new drug to market between $300 million and $4.5 billion, to feasibly produce new drugs and continue the innovation process, pharmaceutical firms often prioritize producing treatments which require continuous use or for prevalent diseases that affect a large portion of the population. (2)
While curative treatments provide pharmaceutical companies with a “single-time” profit, treatments offer sustained revenue over time. However, this same idea might apply to the actual diseases treated themselves. Why spend capital developing a curative treatment for an acute disease when the alternative is providing a long-term treatment for a chronic disease such as diabetes, asthma, or Alzheimer’s?
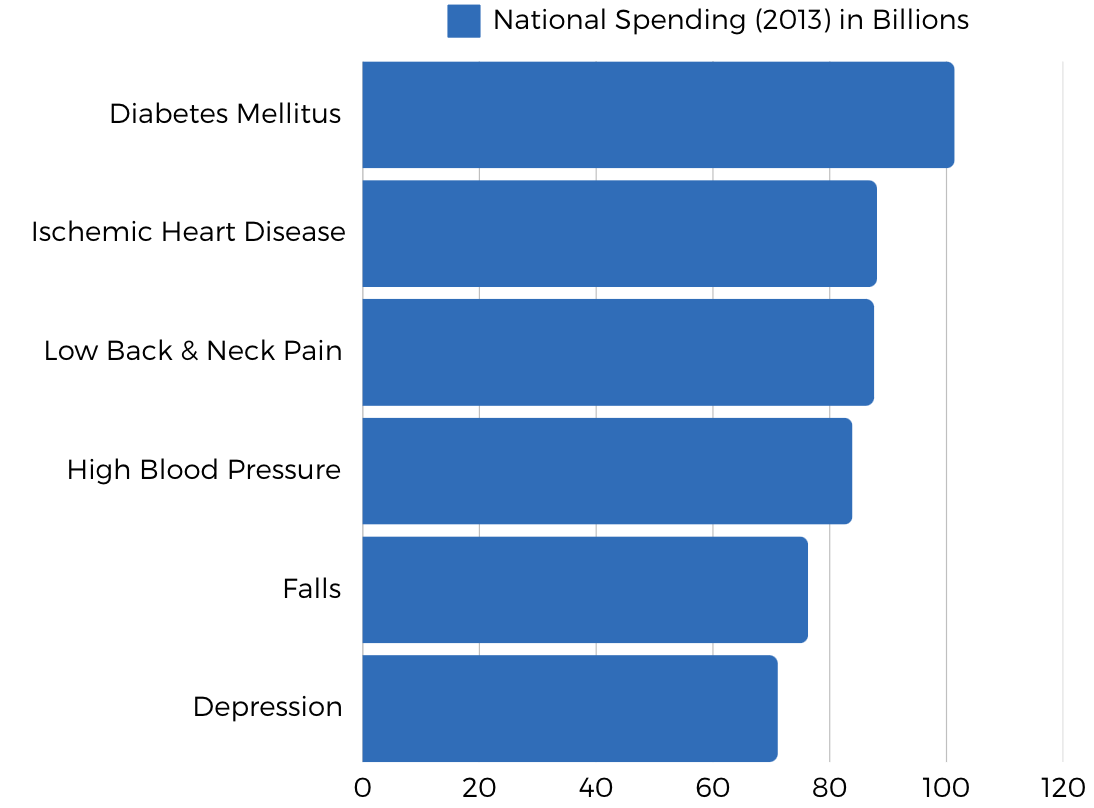
While this trend does align with U.S. spending data (5 out of the 6 most funded disease-states in 2013 were chronic), national spending does not necessarily align with pharmaceutical incentives and more often reflects patients’ and government priorities. (3)
You might be wondering: what about those rare conditions that affect a very small proportion of Americans? These “rare” or “orphan” diseases, such as cystic fibrosis, Huntington’s, and sickle cell disease, are not commonly funded (at least at first) by large pharmaceutical companies. (3, 4) These diseases tend to be investigated by smaller companies with lower overhead costs since the likelihood of receiving immediate and large profit from rare disease exploration tends to be low. (4) These companies, after identifying a potential curative or ameliorative therapy, tend to be purchased by larger pharmaceutical brands which then market and further develop the product. (4)
Ultimately, we, as patients, do not have much control over what diseases receive the most governmental and research funding or what drugs actually end up reaching the market. In this nation’s capitalist system, market forces and corporate incentives determine what diseases are explored and what drug types are available to consumers. However, a new model has emerged in recent years to provide patients with a voice in drug development -- PFDD (patient-focused drug development). (5) Implemented by the FDA’s Center for Drug Evaluation and Research, this initiative attempts to include patients’ needs and voices into the pharmaceutical decision-making process; this occurs by expanding clinical trial enrollment, understanding patient preferences, increasing communication of potential therapy risks, and allowing patients to guide pharmaceutical production. (5) From 2012 to 2022, over 24 PFDD meetings were held, with administrators reporting substantial improvement regarding patient-centered pharmaceutical development. (6) Ultimately, while the capitalist system in the U.S. tends to support profitability over quality and affordable medical care, programs like the PFDD might allow us to re-align incentives ensuring that pharmaceutical companies work to support the public health of this nation.