- Health in Perspective
- Posts
- But is it “Medically Necessary”?
But is it “Medically Necessary”?
Prior Authorization and Insurance Coverage
Vinay Sudarsanam
December 25, 2024

Your condition is not “severe” enough. The treatment requested is too costly. The documentation is incomplete. The treatment requested is not “medically necessary.” The topic of health insurance coverage has been in the news frequently, so why and how do insurance firms decide what to cover?
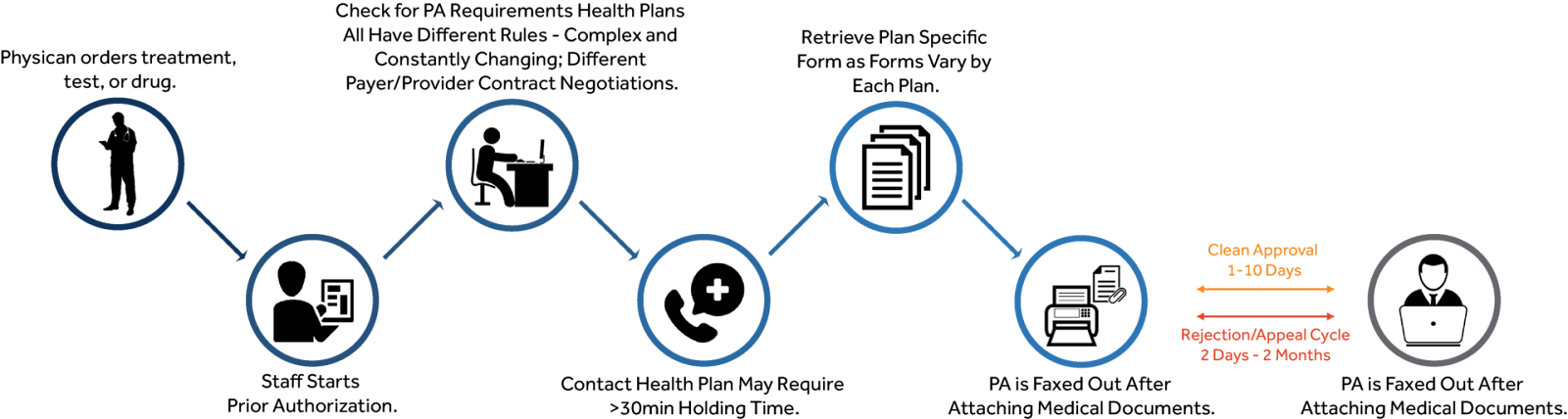
Health insurance plans rely on a process known as prior authorization to restrict the care an enrolled person can receive. (1) So how does this work? Essentially, a healthcare provider must first document the treatment they intend to provide the patient before the patient receives care; at this point, the patient’s health insurer reviews the intended treatment along with other documentation to ensure that said treatment is medically necessary and a good use of healthcare resources. (1) This process is depicted in the graphic below. (2)
The potential pitfalls of prior authorization have been widely documented in the media. However, before I discuss these, it is important to note that not all health insurance plans use prior authorization. While prior authorization tends to be used only in some government health insurance plans and in managed care plans, a 2024 survey found that 48% of all insured adults were registered in plans that required prior authorization for a procedure in the year preceding the survey. (4, 5) So what are the real-world consequences of prior authorization and how does the appeal process affect healthcare providers and patients?
A 2024 study from the American Medical Association identified that by 2034, there will be a physician shortage of at least 30,000 in the U.S. (6) Physicians, thus, have to carefully balance their time providing care to patients and completing administrative work.
Prior authorization, as expected, significantly changes that balance; it is estimated that prior authorization results in increased administrative expenditures of $35 billion annually. (7) A 2024 report found that physicians spend approximately 2 hours completing administrative work for every hour providing patient care; prior authorization thus hinders the amount of time that physicians can spend treating and supporting patients. (7) Sending prior authorization forms and completing requests costs about $11,000 per healthcare provider per year; this increased administrative workload has real consequences for the American healthcare system as 95% of physicians have stated that authorization procedures have increased feelings of burnout. (7, 8)
Ironically, prior authorization does not streamline healthcare; contrary to its main purpose, the process actually accelerates inefficiencies within the system, increasing physician burnout and reducing the amount of time providers can spend actually treating patients.
Beyond increasing administrative workload, prior authorization processes have real consequences for patients. Prior authorization is required for a vast majority of healthcare services; in a 2023 American Medical Association survey, over 50% of surveyed physicians reported requiring prior authorization to prescribe a generic medication. (8) This results in significant delays in care; in the same study, 88% of physicians claimed that prior authorization procedures hindered care continuity and about one third of all physicians report that a serious adverse event had occurred as a result of a delay in care due to prior authorization. (7, 8) Importantly, in 2023, 42% of physicians reported that prior authorization procedures resulted in an emergency care visit. (8)
Beyond delays in care, prior authorization may also expand disparities in access to treatment; each insurance firm (United Healthcare, Blue Cross Blue Shield, Aetna, Cigna…) conducts its own authorization process. Thus, for a single condition, different insurance plans may authorize different treatments resulting in different outcomes for patients. This prior authorization process also occurs at the discretion of the insurer and not the provider; ultimately, the physicians and administrators employed by insurers who are conducting the approval process may not understand the full situation, contributing to poorer patient outcomes that reflect poorly on the patient’s physician.
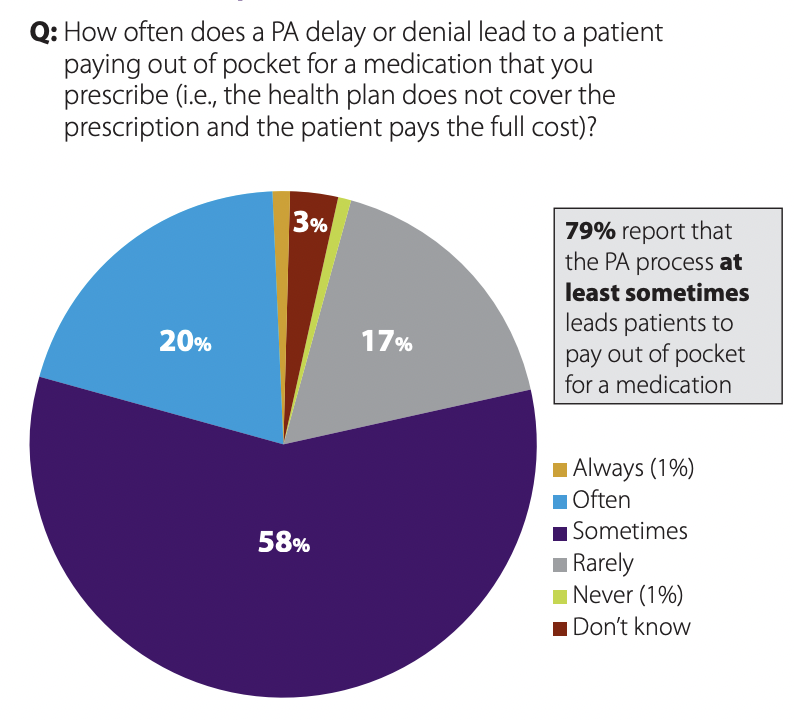
In fact, a prior authorization denial may result in no insurance coverage for a particular healthcare service. This might result in patients paying out-of-pocket for that service; a chart depicting the frequency of prior authorization denials and out-of-pocket spending on healthcare services is depicted below using data from the 2023 physician study. (8)
Each prior authorization denial may result in longer wait times for patients as they must work with their provider team to re-apply for coverage with the possibility of never receiving coverage for that treatment at all. This runs contrary to the point of health insurance as enrolled patients pay monthly premiums yet may not receive comprehensive coverage for previously agreed upon services and may be forced to pay significant out-of-pocket costs regardless of coverage.
As I mentioned before, cost-savings and efficiency data with prior authorization processes are mixed at best; however, due to an abundance of literature showing the adverse effects of insurance coverage denials on patient outcomes, the federal and state governments have decided to limit prior authorization in some cases. (1) The ACA prevents the use of prior authorization in emergency medicine and several states, including New York, are limiting the use of prior authorization for behavioral or mental health services. (1)
The topic of prior authorization is complex and while many online have recommended increased transparency regarding insurance denials as a potential solution, transparency itself does not solve the root cause of the issue. Prior authorization has hindered the effectiveness of healthcare providers resulting in patients being denied care recommended by their providers but not by their insurance firms.
The goals of prior authorization include reducing healthcare costs and protecting against fraud and overprescription of expensive therapies; however, health insurance administrators are often unaware of a patient’s complete story while their provider may have a more comprehensive understanding of their patient and their medical history. Ultimately, to reduce conflicting priorities, it is important to expand internal hospital safeguards against overuse of medical services rather than leaving those safeguards up to insurance companies which have a vested interest in reducing healthcare costs to protect their bottom line.