- Health in Perspective
- Posts
- Similar Systems Different Results

This post is the first describing my journey to Rwanda and Uganda. While I will eventually explore resource and administrative inefficiencies in decentralized healthcare systems as well as the difficulties faced when providing care to underserved and isolated populations, this article will primarily focus on the differences between Uganda and Rwanda. The main point is this: while these two countries have fairly similar decentralized healthcare systems, a multitude of factors ultimately influence healthcare outcomes and contribute to disparate outcomes between the two countries.
Rwanda is widely seen as having one of the best healthcare systems in Africa. (1) Citizens receive healthcare for roughly $2 per year (keep in mind that $1 USD equals about 1300 Rwandan Francs). The Rwandan government subsidizes the rest of this per patient cost - roughly $10-15 per year. The Rwandan healthcare system operates through a simple referral network: patients receive most services at a local health center; for more specialized treatment, they are referred to a district hospital and then a referral hospital. At this highest level of care - the referral hospitals, the University Hospital of Butare, University Hospital of Kigali, Rwanda Military Hospital, and King Faisal Hospital provide patients with the most specialized treatment. (2) This system stands in contrast to private insurance where patients pay out-of-pocket for specialized hospitals.
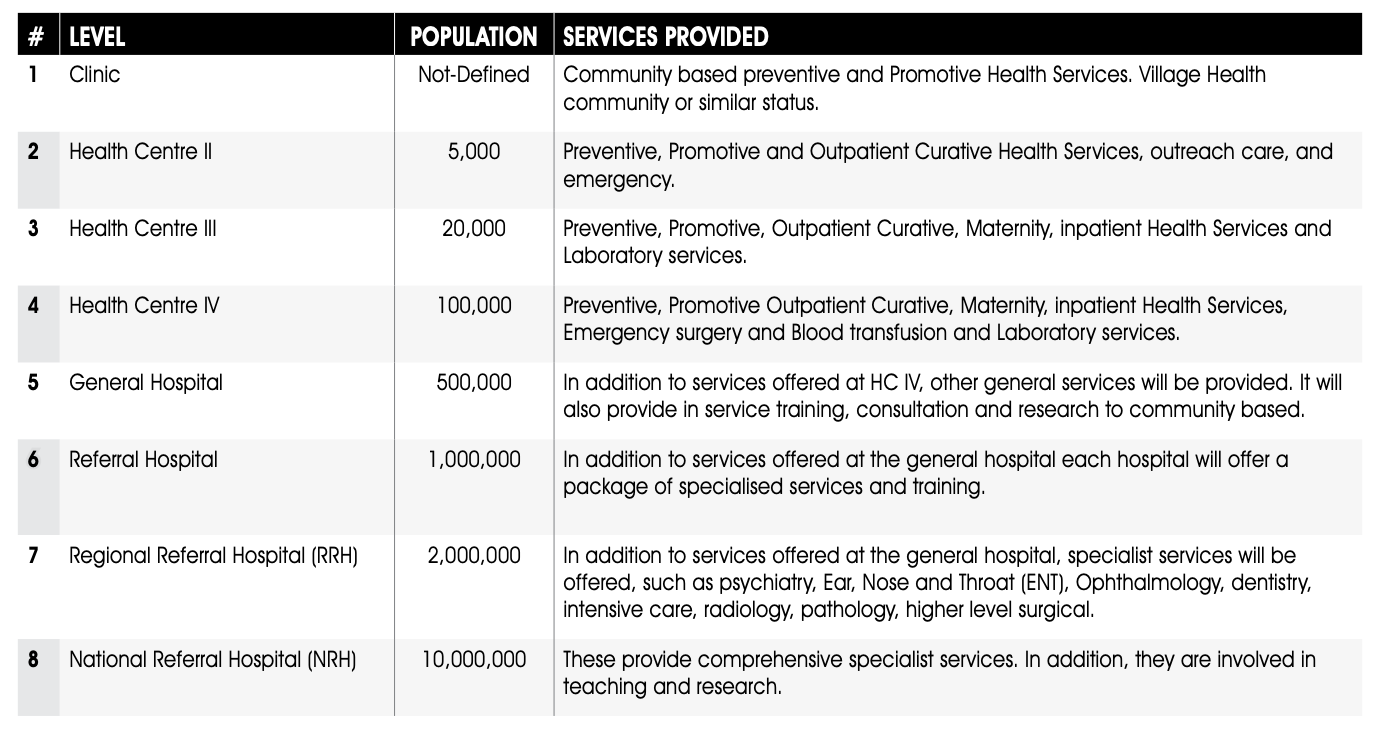
While Uganda has a similar decentralized healthcare system with patient referrals to more specialized care, the patient experience and outcomes differ significantly. Patients first access care at Level 2 Clinics which are generally led by community workers; often, these clinics are understaffed or are insufficient in resolving patient needs. If the patient’s needs are not resolved, they are referred to a Level 3 Clinic, led by a nurse and which generally serves a larger patient population. From there, patients may be referred to a Level 4 Clinic, operated by a physician. For more complex cases, patients may be sent to a District or General Level Clinic, a Referral Clinic, a Regional Referral Clinic, or finally the National Referral Clinic (in the capital city of Kampala), all of which are operated by a team of physicians. If this sounds complicated, it is. This decentralized system in Uganda, which in concept prioritizes patients with more debilitating illnesses, results in resource gaps between regions and creates a trickle-down effect where fewer and fewer resources reach the more community-level 2 or 3 Clinics. (3)
This idea of resource disparity and maldistribution is complex and hopefully you will get a better picture of what I’m talking about over the next few articles.
The first part of this that I hope to discuss is administrative priorities. While over 90% of Rwandese individuals were insured in 2020, only 500 thousand Ugandans (~1.1%) were insured in a recent report. (4,5) In fact, while in Uganda, I learned that the government had reallocated roughly 300 billion Ugandan shillings (~$81 million USD) from healthcare to the Bank of Uganda, further indicating a priority shift away from healthcare. (6)
This strategy of increasing healthcare options for individuals with more complex illnesses seems like a viable way to conserve scarce medical resources. However, with the Ugandan population quickly rising and as more and more patients present to lower Level Clinics, these facilities have seen an immense strain on existing staff and resources. Let’s look at Bwama Health Center 3 on Uganda’s Lake Bunyonyi. As depicted on the map below, this clinic is unique in that it serves patients living on or near the many islands of Lake Bunyonyi and provides care for patients with acute conditions via a small ambulance boat.
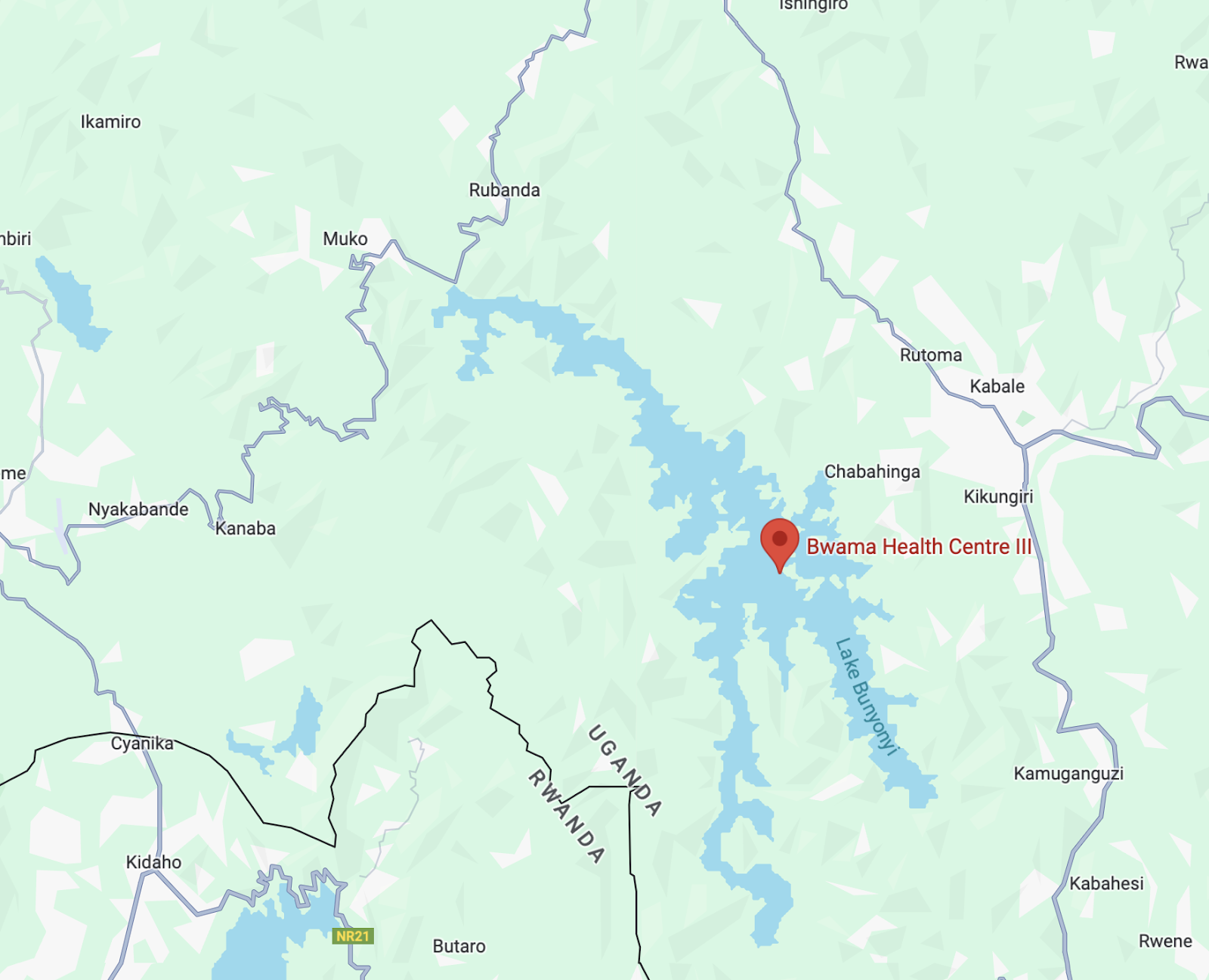
This is Bwama Health Center which was, at the time of my visit, led by a team of medical students and nurses from Slovenia. (7)

This health center (a Level 3 Clinic) is intended to serve 20 thousand patients. Furthermore, as the Ugandan population continues to grow, access to care will only diminish for patients in this region. However, this crisis does not pertain only to the lowest level clinics. Take Kabale Regional Hospital, designed to serve roughly 2 million patients as the largest teaching hospital and medical center in the region, and which possesses only 3 operating rooms to handle C-sections and complex medical procedures. (8)

While I was not able to spend much time in Rwanda to learn about the nation’s healthcare system, those I spoke to were immensely satisfied with the cost and quality of healthcare. The universal insurance model covers patients’ most basic needs and the government appears willing to invest in citizens’ health. A prime example is cervical cancer: in 2011, Rwanda implemented a national HPV vaccination campaign for schoolgirls, reaching over 90% coverage across the nation since then. (9) As cervical cancer and other previously common diseases become less of a concern in Rwanda, these issues are still felt in Uganda, a neighboring country.
While the decentralized healthcare systems of Rwanda and Uganda both operate through a patient referral system with multiple levels to access care, patient outcomes differ largely due to administrative influence and resource allocation. While Rwanda’s universal healthcare insurance approach guarantees patient satisfaction and access to basic care, Uganda’s complex level system has resulted in a reduced trickle down effect whereby patients who present at lower level clinics often leave without resolution to their health issues. Although the differences between Uganda and Rwanda seem stark (and I hope to explore both nations in the future), my future articles will primarily explore the complexities of healthcare in Uganda, focusing on resource distribution and the provision of care to isolated communities.