- Health in Perspective
- Posts
- Policies of Prevention

**IMPORTANT: This article contains mentions of cervical cancer. If you feel uncomfortable with these topics, please refrain from reading.
Cervical cancer is a complex disease that presents unique public health challenges in different nations. Lower and middle-income nations especially have struggled tackling this disease from a prevention standpoint, focusing instead on diagnosis and subsequent treatment. However, new data has presented new solutions to tackling cervical cancer from a health systems approach. A January 2024 study from Scotland has identified that a new national HPV vaccination and cervical cancer screening program immunizing girls aged 12 and 13 years old and starting in 2008 has effectively reduced cervical cancer cases to zero. (1)
Cervical cancer prevalence is rising both in the US and around the world with growing disparities between lower- and higher-income nations: when corrected for hysterectomies, cervical cancer rates are 14.1 and 9.5 per 100,000 people in low- and high-income nations respectively. (2) From a health system perspective, what might contribute to this disparity in disease prevalence and what can we take away from the Scotland case study as to how we might reduce cervical cancer prevalence moving forward?
As is the case when treating nearly any disease, health system interventions generally target disease prevention, early stage disease, and late stage disease.
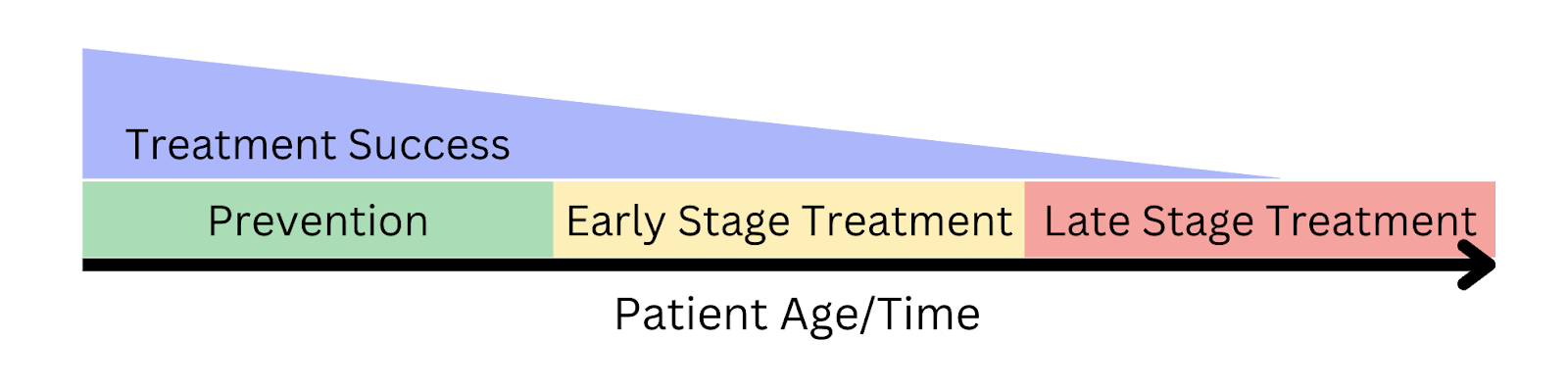
Patients might receive care before they are diagnosed with a disease, while the disease is in its initial stages, or when the disease has progressed into a later-stage. However, treatment is generally most effective and cost-efficient at the preventative stage; when disease is treated proactively, patients may reduce the likelihood that they acquire a disease without ever experiencing symptoms. One of the most problematic aspects about cervical cancer is that the disease is hard to identify in early stages. (3) Thus, treatment must focus either on prophylactic treatment before the disease presents in the first place or new tools to detect cervical cancer must be developed.
Furthermore, because cervical cancer screening is so resource intensive, disparities in healthcare resources become correlated with disparities in healthcare outcomes. While higher-income countries might be able to develop the resources necessary for a universal vaccination program like Scotland’s, lower and middle income countries where cervical cancer is much more prevalent may not have the resources necessary to implement similar programs. (4) This problem has resulted in a cervical cancer mortality disparity between nations: nations with comprehensive healthcare coverage and the resources to provide effective preventative treatment have the lowest cervical cancer mortality. (5) In fact, while Northern European nations have a mortality rate of roughly 2.1 per 100,000 individuals, Eastern African nations have a cervical cancer mortality rate of almost 30.0 per 100,000.
Moving forward, what can we take away from the Scotland intervention and can a similar program be used in other nations? The Scotland study relied on the GARDASIL 9 vaccine which was offered to students in their first year of secondary school (S1). These programs have been adapted in the US as well and typically involve school-located clinics that educate students about vaccines and provide options for vaccination. (6) The user convenience of this program makes it efficient to increase vaccination rates in many situations; by supplying vaccines and educating patients in an easily accessible location (such as schools), administrators can maximize the number of doses delivered and thus achieve the best possible outcomes.
The Scotland study also showed that cervical cancer outcomes might be improved even in non-optimal conditions. The intervention demonstrated that vaccinating girls at ages 12 or 13 resulted in a near-negligible number of invasive cervical cancer cases regardless of how many vaccine doses each individual received. The impacts of prophylactic care cannot be overstated: the Scotland case study proves that prevention is one of, if not the, most effective policy avenue for complex disease. While cervical cancer is one of the most prevalent and debilitating cancers in most parts of the world, an effective prevention and screening approach has the potential to reduce the prevalence and mortality of this disease.
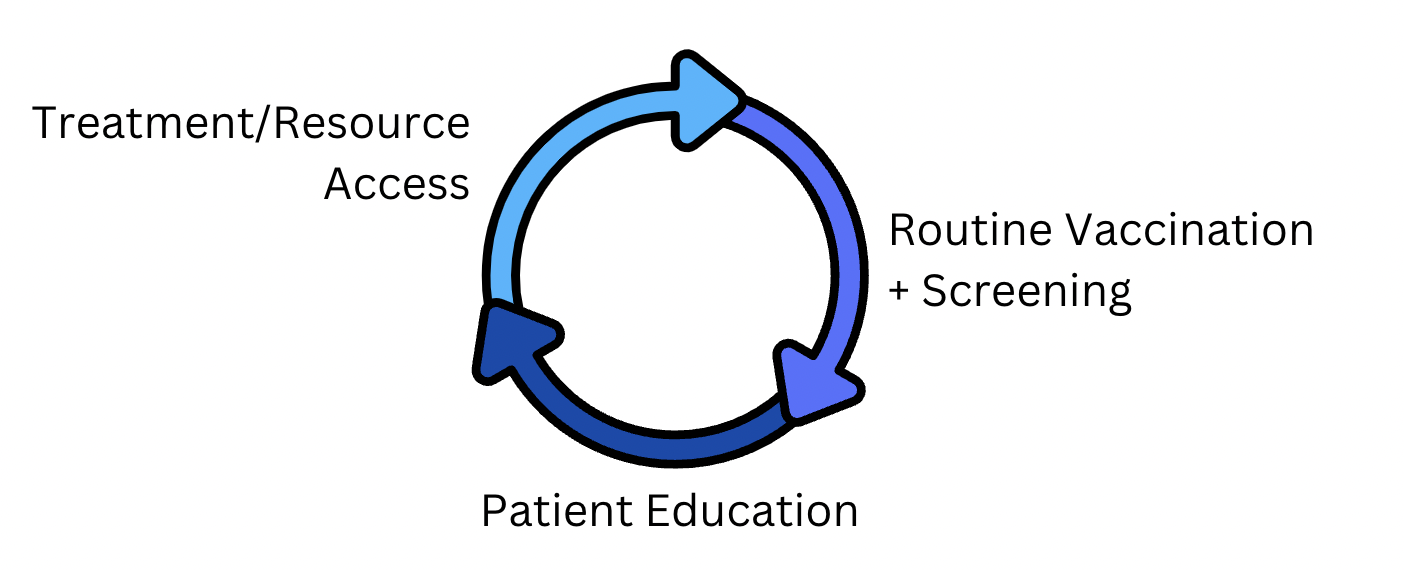
By providing HPV vaccine and cervical cancer education to patients and offering routine vaccination and screening in an easily accessible manner (ex. school-located clinics), public health professionals might reduce the prevalence of cervical cancer once and for all. However, resource access is of the utmost importance when providing prophylactic treatment; I hope to focus on this aspect of preventative care moving forward when discussing international public health efforts.
The Scottish Healthcare System is organized via the National Health Service (NHS), providing universal health care access to all residents. (7) Individual healthcare is funded via taxation of all residents. While HPV vaccines for a large portion of the Scottish population may be feasible within the NHS system, a similar model may not be as feasible within larger private insurance models (as in the US) or primarily out-of-pocket models (as in countries such as India). At the end of the day, a similar intervention might require both an adequate supply of prophylactic resources as well as the ability to provide resources at low or no cost to individuals.
Ultimately, there are two sides of patient care: to provide effective treatment, providers must have novel technologies and therapies, but also streamlined systems to facilitate earlier and better treatment. Cervical cancer is one of many chronic conditions plaguing healthcare systems across the globe; by focusing on reducing disease prevalence via prophylactic treatment and by collaborating directly with local experts and communities in need, public health professionals might reduce structural health disparities and improve outcomes.