- Health in Perspective
- Posts
- Health Crisis Intersectionality

**IMPORTANT: This article contains mentions of food insecurity. If you feel uncomfortable with these topics, please refrain from reading.
In the US, we often do not think about food insecurity as an issue or one that affects a large number of people: it may then come as a surprise to hear that 54 million people in the US (about 16.3% of the population) are currently food insecure and that 23.5 million people (about 7%) live in food deserts. (1)
Before I continue with this article, I hope to differentiate between two terms: food insecurity and food deserts. Food insecurity is generally defined as having a lack of access to enough food that satisfies the nutritional needs of all members of a household. On the other hand, a food desert is a geographic region and households in that region typically lack access to nutritious food either due to cost or because stores that offer such food are far away.
Defined by the Healthy Food Access for All Americans (HR 1313) Act, the term “food desert” has been used for years to describe regions of low-access and low-income, compounding factors that result in poorer health and nutrition outcomes. (2) However, in recent years, the term has fallen into controversy with many advocating that the term should be changed. (3) While some argue that the term minimizes the efforts taken by individuals in food deserts to identify nutritious food, others argue that the term hides the fact that these deserts are “man-made”, a product of policy.
Regardless of the term however, the statistics are shocking: data from the American Community Survey suggests that roughly 12.8% of the US population (39.5 million individuals) are currently living in low-income and low-access areas (or food deserts); furthermore, roughly 6.2% of the population (19 million people) have limited access to local healthy food options. (4)
Where are “food deserts” in the US?
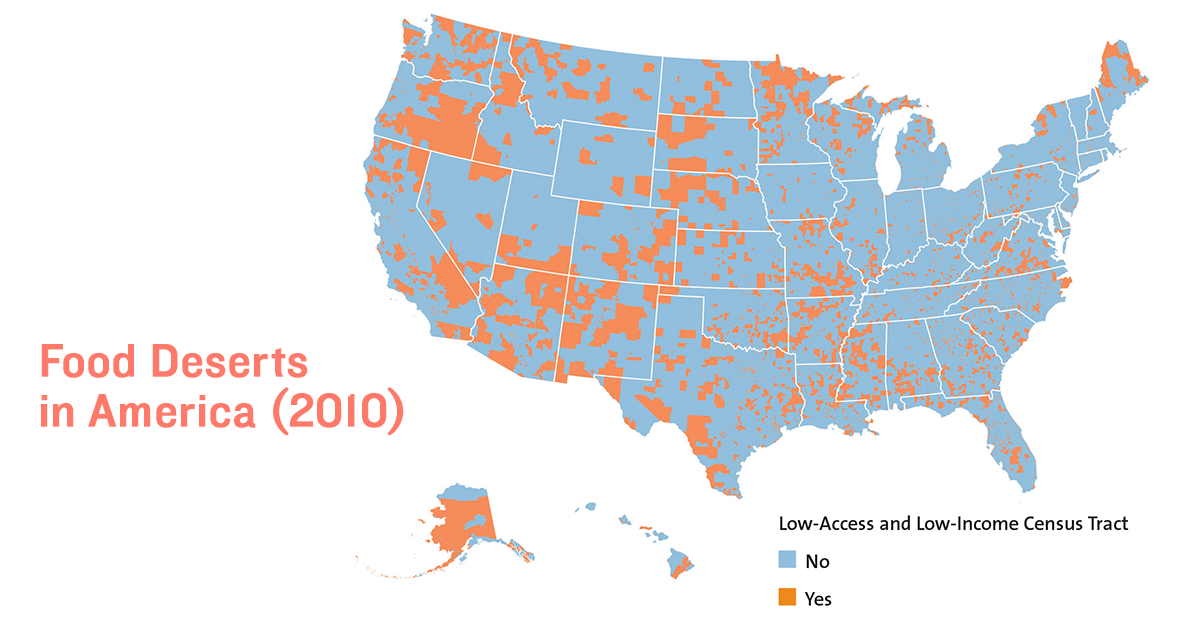
Enterprise Community Partners released this Food at Home report to describe areas of low-income and low-access using very specific definitions for each term. Low-access regions were defined as locations where, in order to reach a store that sells nutritious food, at least one-third of all residents must travel at least 1 mile in urban areas or 10 miles in rural areas. Furthermore, low-income areas were defined as regions with a local poverty rate of 20% or more or regions with a median household income of 80% of the statewide median or less.
Clearly, food insecurity is a prevalent issue in the US; the COVID pandemic only exacerbated this problem with food supply chains falling apart and a greater share of the population becoming unemployed.
Living in a low-access low-income region increases the likelihood of developing physical and mental illnesses over time.
Individuals living in food deserts lack access to nutritious food, often resulting in poorer diets consisting of mainly processed foods. (5) Limited access to nutritious food increases the likelihood of developing obesity, especially by consuming foods high in fat and sugar. (6)
Individuals consuming highly processed foods are also at greater risk of developing chronic illnesses such as diabetes and cardiovascular disease.
Finally, individuals in food deserts where even processed food is scarce often experience additional stress as they try to identify new sources of food. (7) Chronic stressors often have long-lasting effects on mental health.
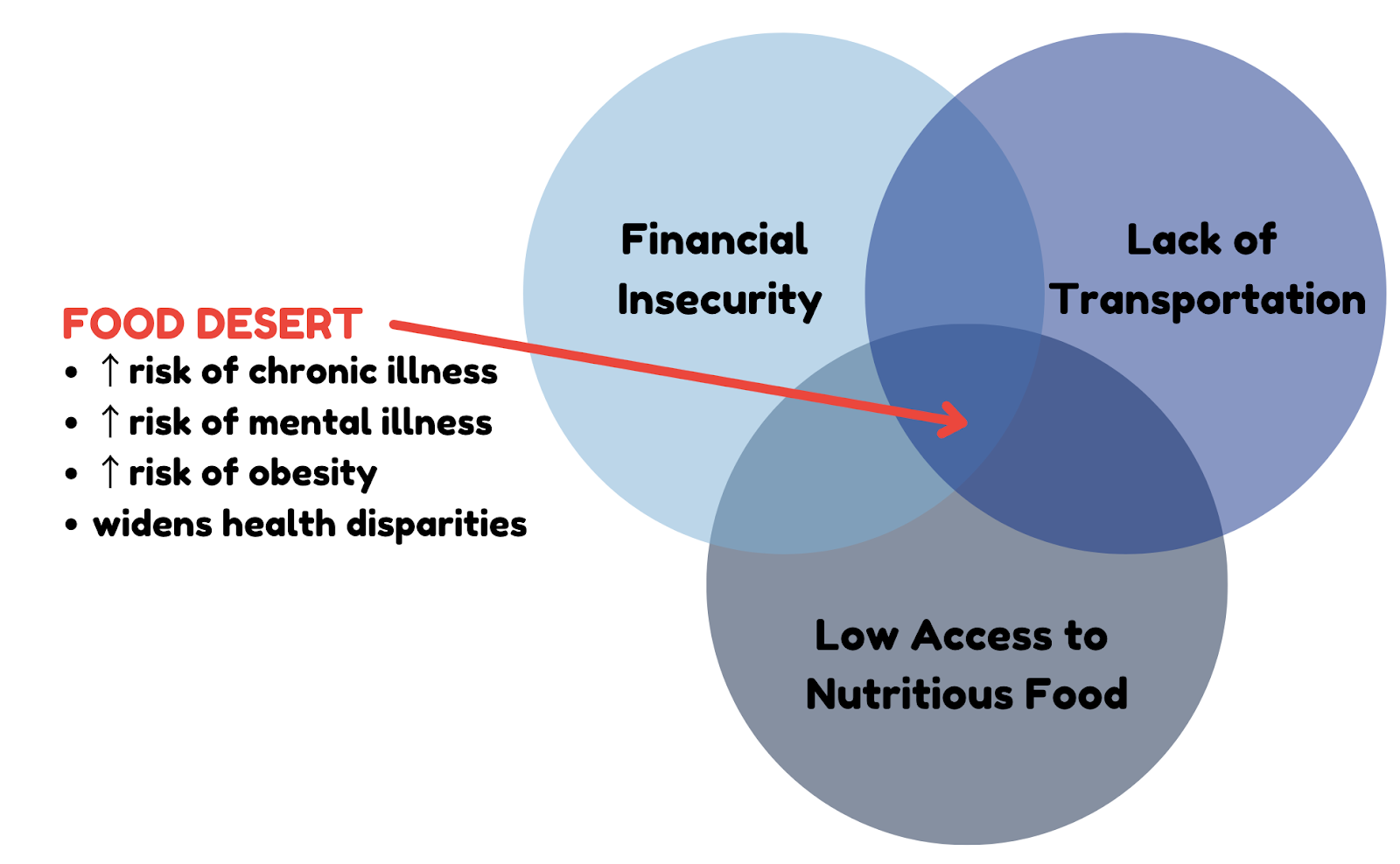
The Venn Diagram I present above illustrates the true magnitude of this issue and reflects a recurring problem when analyzing health disparities. Individuals affected by health issues most severely are often affected by the “intersection of” or a multitude of different issues combining to form a larger problem. In this case, a lack of nutritious food nearby, coinciding with the inability of individuals to pay large sums of money for food, and a lack of transportation infrastructure create food deserts: a larger and more pressing issue than food insecurity caused by a single factor alone.
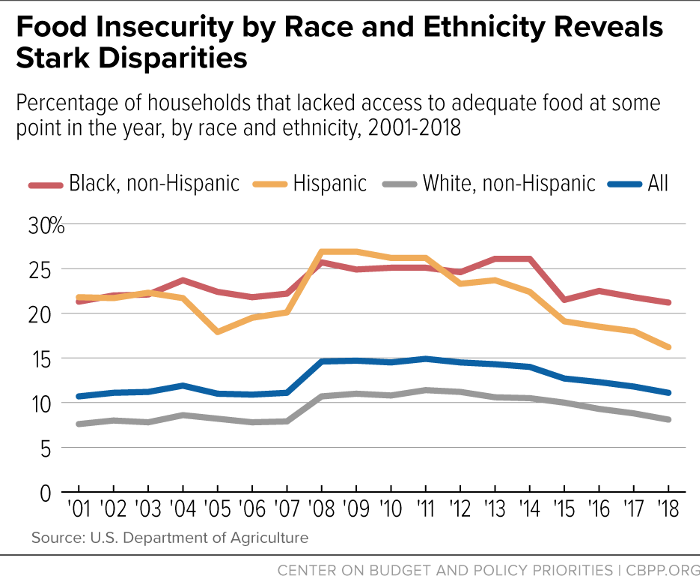
While food insecurity is an issue in and of itself, lack of access to nutritious food in certain geographical regions also plays a role in widening existing health disparities. In this article, I will focus specifically on race-based disparities.
Existing research has proven that individuals of various races experience different health outcomes largely due to inequities in social determinants (SDoH). Chronic illness is more common amongst racial and ethnic minorities in the US, and these minorities also experience increased rates of premature death. (8) When faced with an acute health crisis such as COVID-19, racial and ethnic minorities often fare worse; life expectancies in the US fell more sharply for Black, Hispanic, and American Indian/Alaska Native populations compared to white populations during the COVID pandemic. (9) Finally, in terms of access to health services, in 2017, 10.6% of African Americans were uninsured compared to 5.9% of white Americans. (10)
I present these racial disparities in health to highlight how food insecurity or low-access and low-income regions play a role in perpetuating and even widening these disparities over time. Food desert regions are most often inhabited by racial and ethnic minority individuals. (11)
Because food deserts and food insecurity in general are correlated with income, individuals of minority racial and ethnic groups are predominantly affected by this issue. Limited access to healthy food plays into existing disparities resulting in growing racial disparities in health outcomes in the US.
While this issue seems dire, policymakers have been and still are looking for new ways to tackle this crisis. The Food Deserts Act (HR 1230) has been recently introduced to provide grants to state governments so that grocery stores may be created in underserved communities. (12) The Act, established within the Department of Agriculture, focuses on creating a long-lasting community impact with the creation of these stores; to improve nutrition, the stores must also provide healthy staple foods at or below market prices.
Regardless of the policy created, it is clear that any solution to this issue must tackle one of the root causes, be it a lack of grocery stores, a lack of transportation, or on-average lower incomes amongst residents. By ensuring that all individuals have easy access to nutritious food and by prioritizing the elimination of low-access low-income regions, legislators may reduce racial health outcome disparities while also decreasing the prevalence of chronic physical and mental disease.