- Health in Perspective
- Posts
- Reversing the Trend

**IMPORTANT: This article contains mentions of chronic disease. If you feel uncomfortable with these topics, please refrain from reading.
Over the past few decades, life expectancy in most historically wealthy nations has plateaued. (1) In the 1980s, life expectancy in the United States has held steady near the median of comparable nations; yet since then, life expectancy in the US has decreased, becoming more of an exception to the rule. The question remains: what factors might contribute to this global disparity and from a legislative perspective, what steps might be taken to counteract this trend?
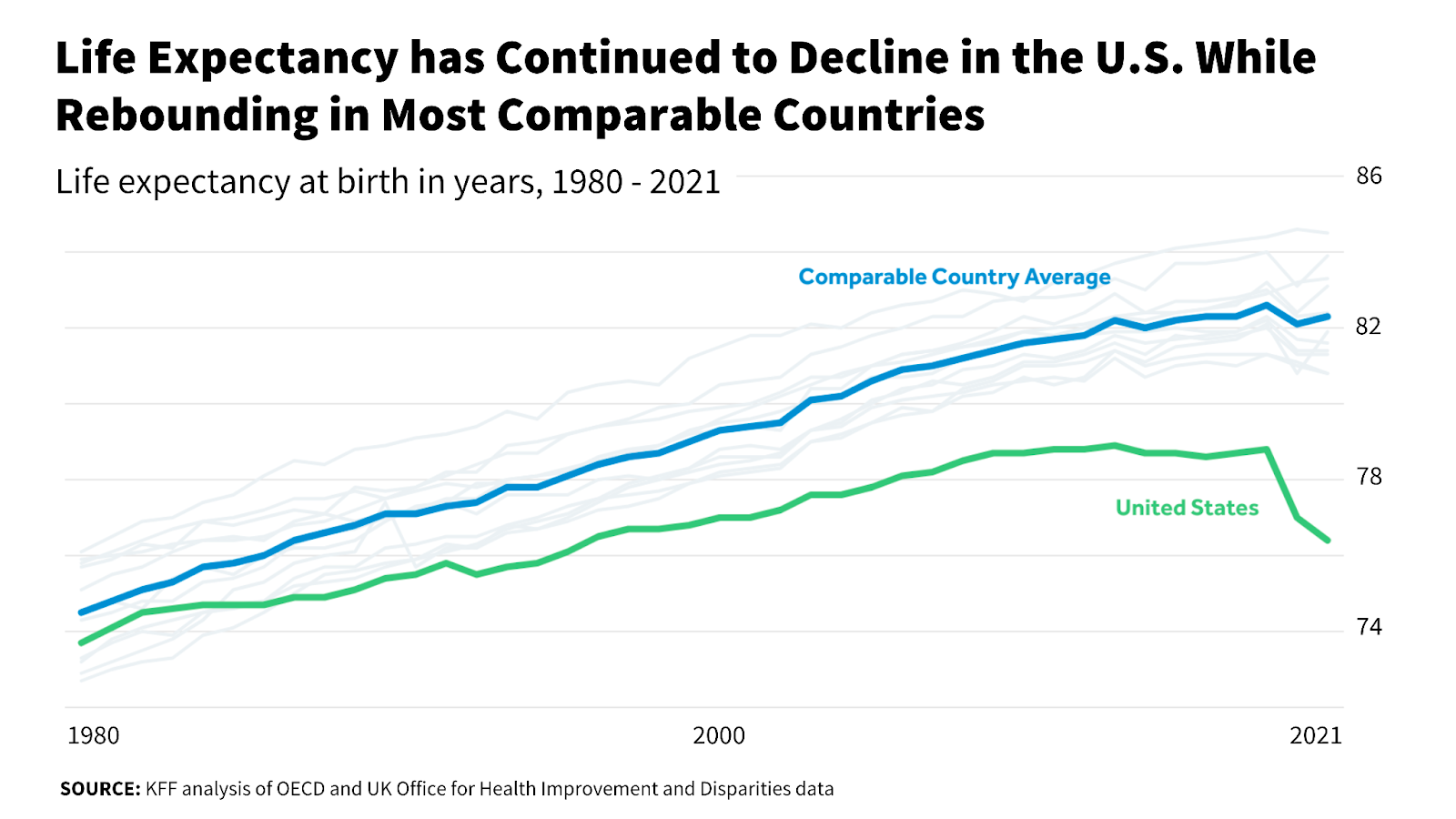
Life expectancy in the US peaked in 2014 at 78.9 years. (2) Since then, life expectancy has hit new lows: CDC NCHS data reports an average life expectancy of 77.0 years in 2020 and 76.1 years in 2021. (3) While the COVID pandemic played a large role in decreasing life expectancy in the US, this trend existed for years before the pandemic began.
Initially, I believed the life expectancy trends in the US and in comparable countries were signs of “lifestyle diseases”: non-communicable diseases, including Type 2 diabetes and cardiovascular disease, associated with modern lifestyles. Yet a recent (October 2023) Washington Post article titled “An Epidemic of Chronic Illness is Killing Us Too Soon” convinced me that this life expectancy disparity might be the result of a more specific issue. In this article, I hope to explain how chronic disease is becoming more prevalent in the US as well as how, from a systems perspective, built heath infrastructure may be at least partially to blame.
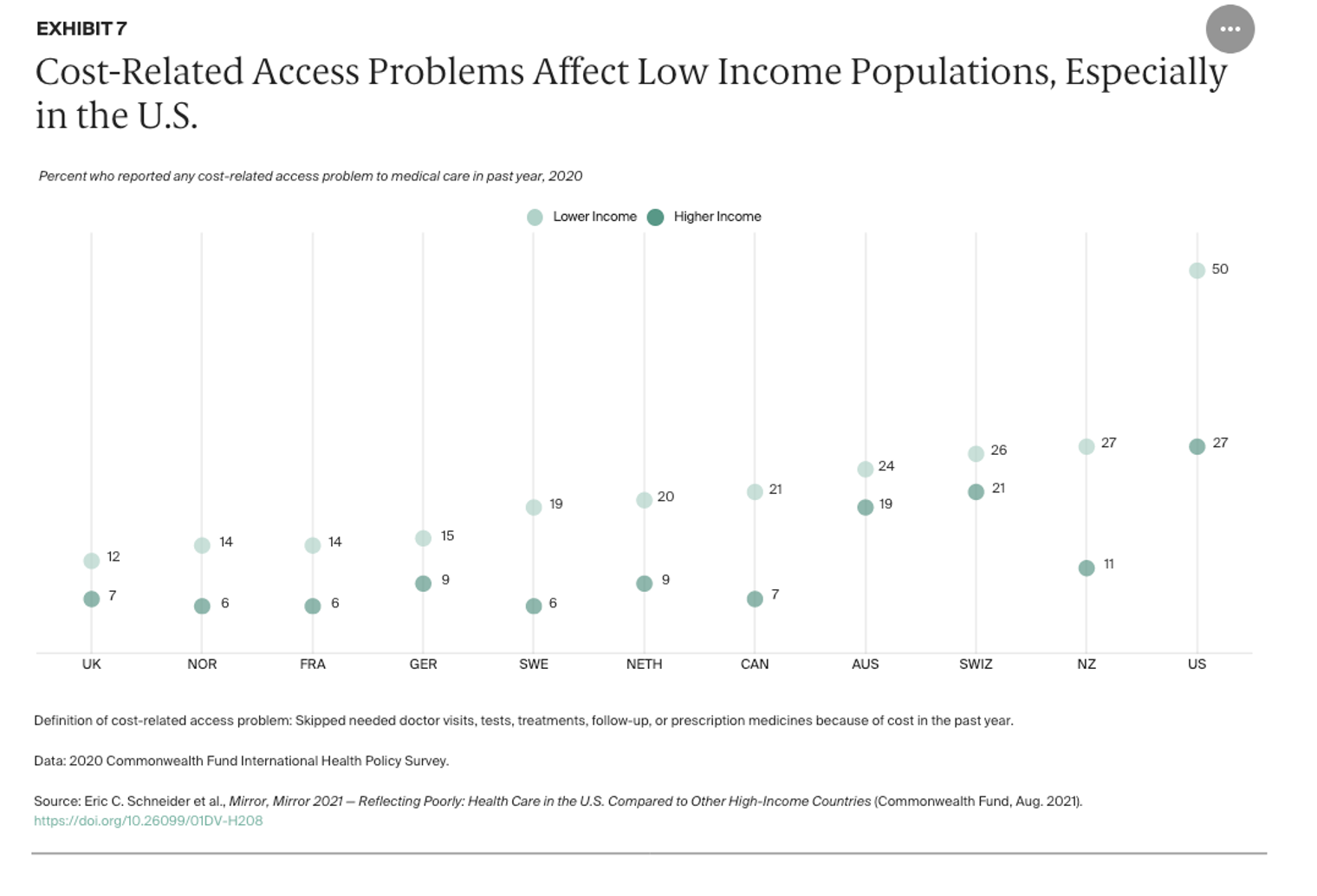
Because individuals in the US must pay for healthcare and health insurance, disparities between higher and lower income individuals have grown faster relative to comparable nations with government funded or mandated health care and health insurance. In fact, compared to other nations, both higher and lower income individuals in the US report significantly more cost-related healthcare access issues.
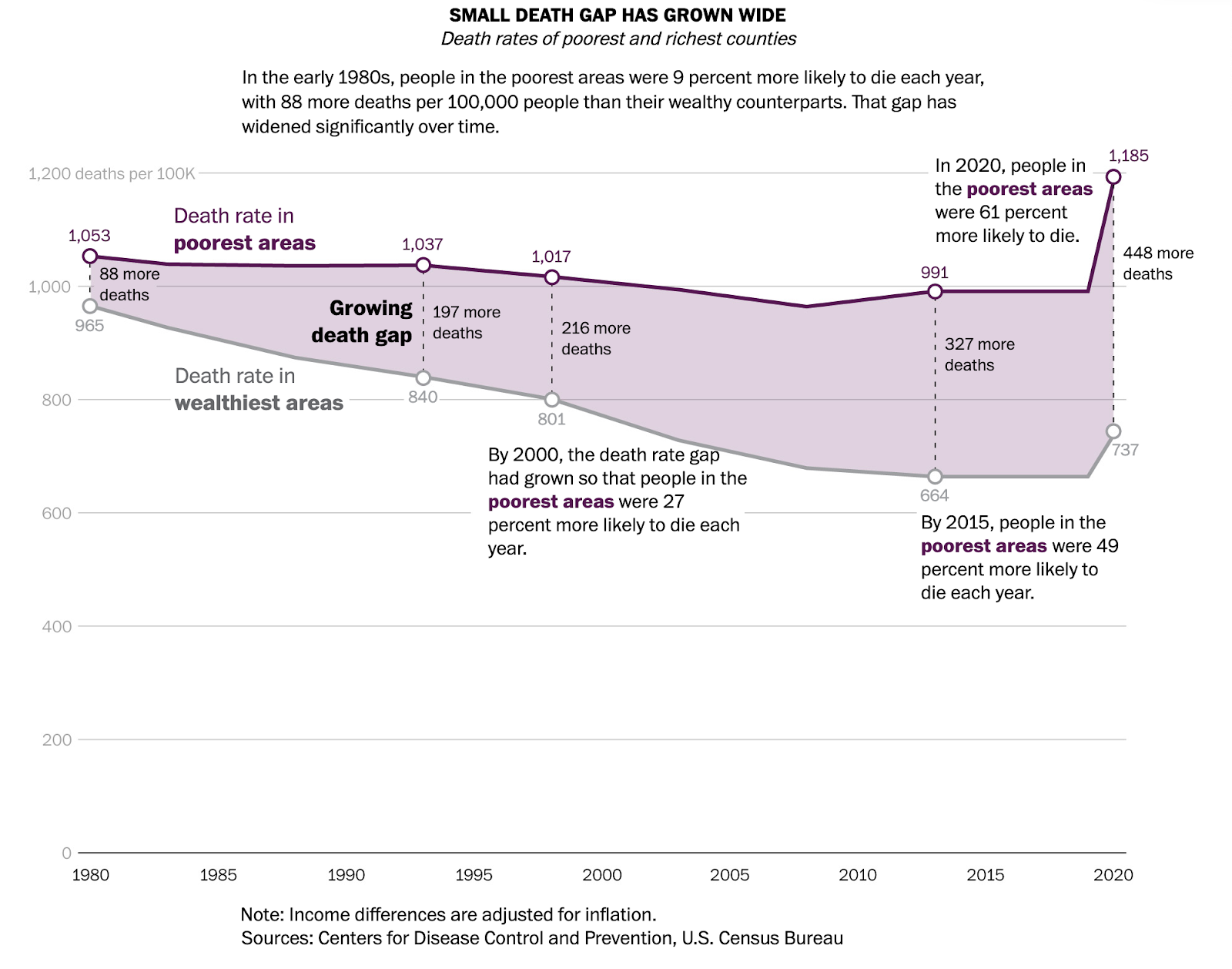
In fact, the Washington Post article documents how, especially in Southern and Midwest states, chronic diseases are killing more people (predominantly between the ages of 35 and 64) than drugs and gun violence. Chronic diseases develop slowly and affect individuals throughout the life course; the most prevalent chronic conditions in the US are cardiovascular, diabetes, respiratory (asthma, pulmonary disease, etc.), obesity, and hypertension.
The Washington Post article cites the increasing prevalence of chronic disease as an indicator of disparity, of “have” and “have nots”. The graph below, provided in the article, shows how, since the 1980s, the gap between the wealthiest and poorest communities have grown, resulting in poorer outcomes.
While healthcare disparities have grown with economic inequity, what is the main driver of health outcomes?
Health is Preventative
High healthcare costs in the US have resulted in a largely reactionary system from a patient standpoint. Let me explain: if an individual patient is forced to pay a large amount to receive care, they would likely only seek care in the case of illness or injury. Why would a patient pay large sums of money to receive medical attention when they are not truly “sick” yet? A 2020 machine learning study indicated that while the US has the highest healthcare spending per capita when compared to all similar nations, only 8% of Americans “undergo routine preventative screenings.” (4)
An increased focus on preventative care would solve a variety of problems in the US: preventative treatment is far more efficient and cost-effective than late-stage medical or surgical treatment, especially for chronic and life-threatening diseases.
In my previous article “Health vs Healthcare”, I discuss how health insurance firms might benefit from expanding the traditional definition of “health” to incorporate its social determinants, supporting the holistic wellness of patients rather than simply medical care. (5) Chronic disease is influenced by a variety of factors from nutrition and exercise to neighborhood and pollution.
Many studies have documented the effect of income in creating disparities in terms of access to nutritious food and leisure time and minimizing consumption of polluted air and water. However, in the US, there exists no program to ensure relatively equal access to resources essential for good health.
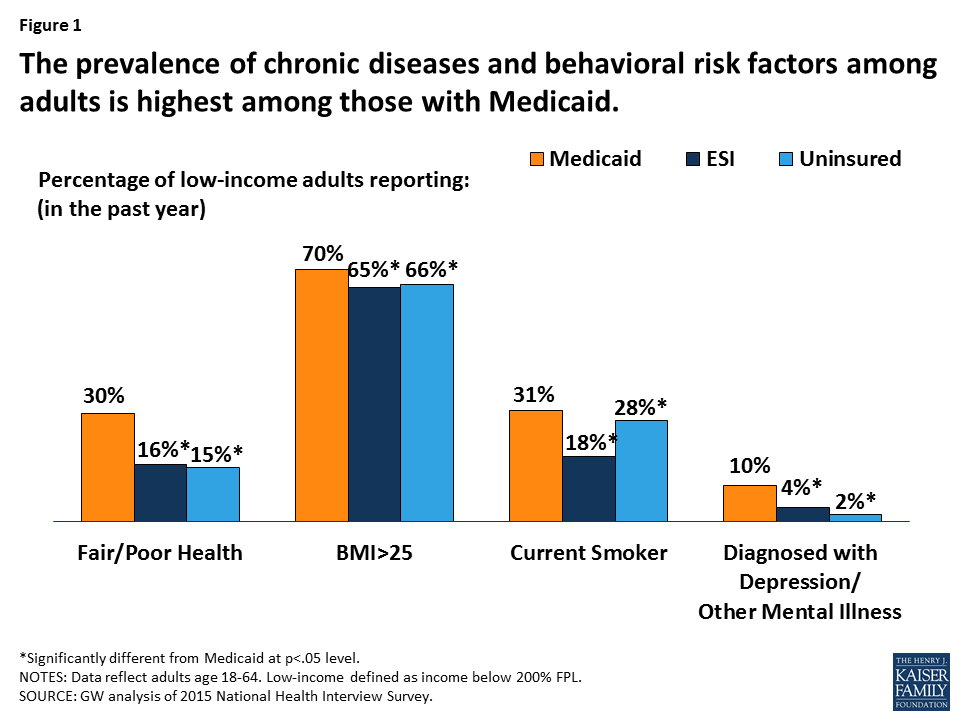
Thus, the risk factors that physicians commonly associate with chronic illness (being overweight, smoking, etc.) are more common amongst lower-income individuals (who are also less likely to be able to access healthcare).
From a policy perspective, this intersectionality of a lack of healthcare access and increased predisposition to chronic illness seems daunting; however, international public health organizations have made strides in reducing chronic disease prevalence in other nations using patient- and provider-friendly interventions.
Since 2018, the organization Resolve to Save Lives has helped expand hypertension (high blood pressure) control and treatment in Bangladesh. (6) Hypertension is one of the most prevalent chronic diseases in the US, resulting in significant mortality. Collaborating with the Ministry of Health, Non-Communicable Disease Control Program, and the National Heart Foundation of Bangladesh, the organization attempted to standardize hypertension treatments, train healthcare workers in supporting hypertensive patients, and reduce providers’ burden of treating large patient populations.
By creating an app for healthcare workers to identify patients’ treatment records, manage drug inventory, and contact patients who miss visits, the organization was able to increase the national hypertension control rate from 20% to almost 60%. Thus, by placing an emphasis on primary care and by collaborating with trusted healthcare service and delivery organizations, Resolve to Save Lives was able to achieve tremendous success in reducing hypertension as one of the leading causes of death in the nation. While this intervention may not work in the context of the US health system, the achievements of Resolve to Save Lives show that progress can still be made to reverse the life expectancy trend we see in the US by decreasing the prevalence of chronic disease.