- Health in Perspective
- Posts
- Care at a Cost

Daylight was fading as I walked out of Kabale Regional Hospital. Crowds of patients stood outside the main entrance waiting for care. As I and a team of physicians began heading for the exit, a young woman ran to us and began speaking in her local language. Immediately after we called a local resident for help interpreting, he recounted to us,
“This woman is giving birth to her 4th child. She was just given a list of supplies to purchase in order to receive care, but she cannot afford them.”
Without hesitation, our lead physician ran to our supplies stock room and brought the items on her list to her for free. The young woman broke down in front of us, thanking the team profusely. Our lead physician visited her after her birth, and due to her immense gratitude, she named her child after the physician.
The ongoing medical supplies shortage in Uganda has resulted in policies mandating that patients purchase and bring specialized drugs and surgical supplies to the hospital prior to receiving care. While this policy raises many ethical dilemmas - including directly ensuring better medical care for those with the ability to pay - in this article, I hope to focus primarily on this policy’s financial and health implications.
The average Ugandan makes around $78 per month. (1) However there is significant variation in earnings. A 1 night stay at a Ugandan hospital costs roughly $20 (not accounting for any medical interventions performed). Patients thus have a significant incentive to avoid the hospital at all costs as a single inpatient stay may result in dire financial circumstances. A 2017 study quantifies this issue, finding that 53% of households borrow money, 21% sell their belongings, and 17% lose a job as a consequence of receiving medical care. (2)

In my previous article “Similar Systems Different Results,” I discuss the ongoing trickle down effect where scarce resources are unequally distributed between large referral hospitals and fewer and fewer “trickle down” to more community-oriented clinics. However, pushing the responsibility of finding and paying for scarce medical supplies to patients punishes patients more than everyone else for resource misallocation at the clinic and governmental level. This policy also increases the variability in healthcare outcomes between communities, as well-resourced hospitals with the capacity to provide patients with essential resources decrease the financial burden of care experienced by patients.
However, this issue is more widespread than you might think. A 2018 report found that over 80% of Ugandan health centers were out of at least one important medication. (3) The report also indicated a prominent lack of vaccines and medications for chronic diseases.
The annual National Health Expenditure Reports released by the Ugandan government break this down even further. (4) The following pie chart shows the distribution of out of pocket expenses for patients in the years 2010-2013; paying for medicine accounts for the vast majority of expenses, with hospital fees and transport also accounting for a significant percent.
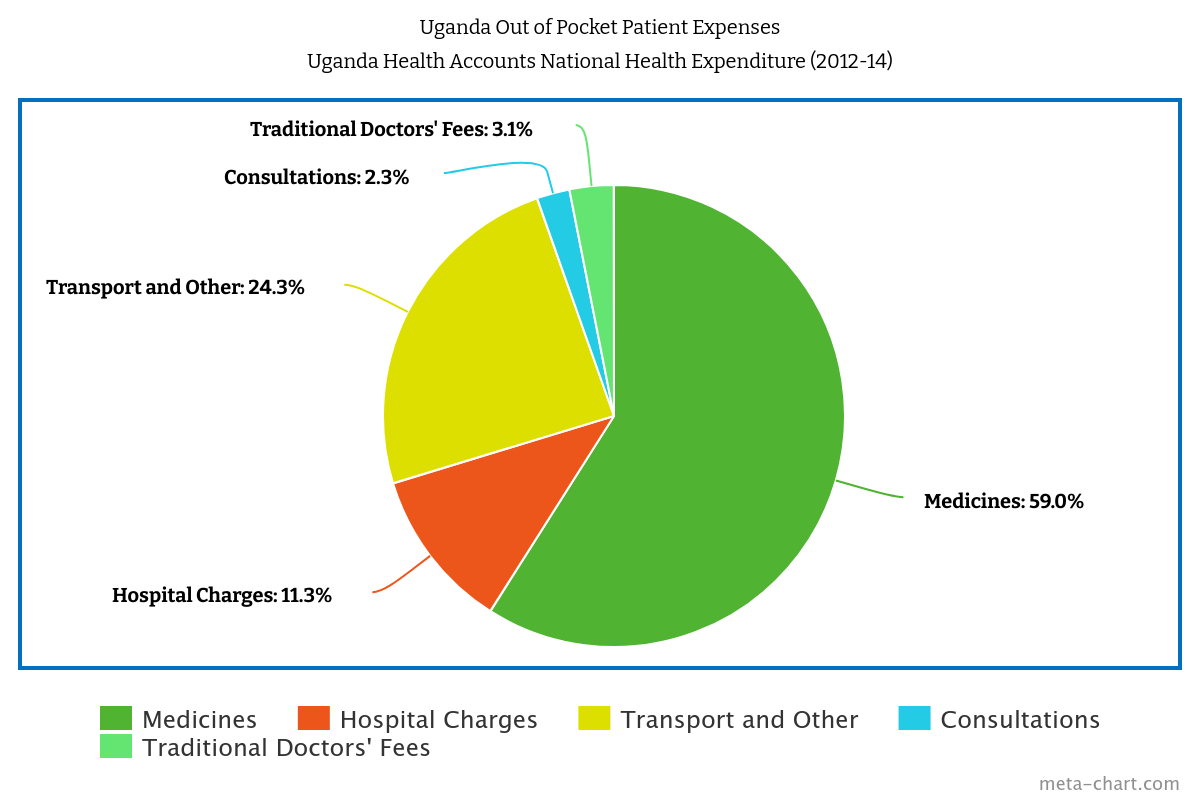
Notably, officials found that malaria accounted for 31% of household health expenditure during this period. The prevalence of malaria amongst the Ugandan population as well as the scarcity of supplies for preventative and acute care (including vaccines, insecticides, nets, and pills) result in many Ugandan households spending large sums of money to protect themselves against the disease. However, this inevitably results in an outcomes disparity whereby individuals who are unable to afford expensive preventative care and disease treatments suffer poor outcomes.
The young woman we met outside Kabale Regional Hospital that day gave birth to a healthy child and left the hospital content and grateful, yet the experiences of so many others who may present to the hospital with acute or chronic issues and lack the ability to pay for scarce medical supplies highlights the issues associated with requiring patients to pay for medical resources before receiving care. The idea that an out-of-pocket expense is a prerequisite to quality medical care exacerbates socioeconomic divisions within the Ugandan population contributing to variability in healthcare outcomes. Resolving this issue requires a concerted effort by government officials, medical and pharmaceutical suppliers, and hospital administrators to reduce resource scarcity and ensure the costs of scarcity do not fall solely upon the patient.